
Hoof Wall Cracks in the Horse: Classification, Assessment, Management and Prognosis
- Marc Jerram

- Dec 30, 2025
- 9 min read
Introduction
Hoof wall cracks represent one of the most common, yet complex pathologies encountered in equine farriery practice (Parks, 2012; O’Grady and Poupard, 2013). They range from superficial cosmetic defects to severe, painful lesions capable of compromising soundness and athletic longevity (Dyson, 2011). For the farrier, hoof wall cracks demand a sound understanding of hoof anatomy, biomechanics, horn quality, and the interaction between trimming, shoeing, and the forces acting upon the foot (Clayton and Hobbs, 2017). Successful management is rarely achieved through a single intervention; rather, it requires accurate classification, careful assessment of both static and dynamic factors, collaboration with veterinary surgeons where appropriate, and a long-term approach aimed at restoring hoof integrity and balance (O’Grady, 2019).
Prefer an audio version? Listen at the link below:
Anatomy and Biomechanics of the Hoof Wall
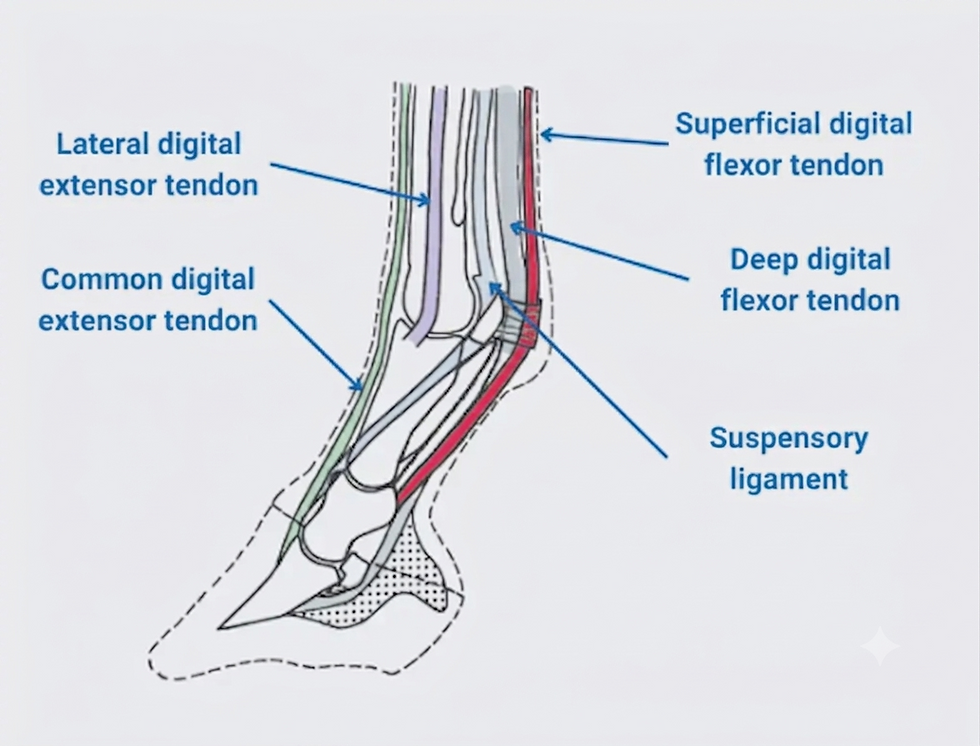
The hoof wall is a specialised keratinised structure designed to bear weight, absorb concussion, and protect internal tissues (Bowker, 2003; Pollitt, 2004). It consists of tubular and intertubular horn arranged in a highly organised pattern, with horn tubules orientated proximodistally. These tubules provide tensile strength, while the intertubular horn binds the structure together (Leach and Zoerb, 2014). The hoof wall is anchored to the distal phalanx by the sensitive and insensitive lamellae, forming the suspensory apparatus of the distal phalanx (Pollitt, 2008).
During locomotion, the hoof wall is subjected to significant cyclical loading. At impact, the wall deforms, particularly at the quarters and heels, allowing energy dissipation (Clayton et al., 2011). Any disruption to horn quality, wall thickness, balance, or loading patterns can predispose the hoof to structural failure in the form of cracks (Parks, 2012). Understanding this biomechanical context is essential when assessing why a crack has formed and how it may be managed.
Classification of Hoof Wall Cracks
Hoof wall cracks can be classified in several ways, most commonly according to their orientation, depth, location, and involvement of sensitive structures (O’Grady and Poupard, 2013). These classifications are not mutually exclusive and often overlap in clinical cases.
Vertical cracks run parallel to the horn tubules and are the most frequently encountered type (Stashak and Hill, 2014). Horizontal cracks run perpendicular to the tubules and are less common but often associated with systemic or traumatic events (Dyson, 2011). Cracks may also be described as complete or incomplete, sensitive or non-sensitive, and by their anatomical location such as toe cracks or quarter cracks. Accurate classification assists in determining severity, prognosis, and appropriate intervention (O’Grady, 2019).
Vertical Hoof Wall Cracks
Vertical cracks originate at either the coronary band or the solar margin and extend along the length of the wall. Their orientation reflects separation along the horn tubules, often due to excessive stress or poor horn integrity (Parks, 2012). Vertical cracks may remain superficial and non-progressive, or they may deepen and destabilise the hoof capsule if underlying causes are not addressed (Leach, 2016).

Vertical cracks are commonly associated with imbalances in mediolateral or dorsopalmar hoof conformation, excessive toe length, under-run heels, or chronic flare (O’Grady and Poupard, 2013). Environmental factors such as alternating wet and dry conditions can exacerbate horn weakness, increasing susceptibility to cracking (Faramarzi et al., 2020). In many cases, vertical cracks are multifactorial in origin, reflecting both mechanical and biological influences.
Horizontal Hoof Wall Cracks
Horizontal cracks occur across the hoof wall, interrupting multiple horn tubules. They are frequently associated with a disruption to horn production at the coronary band, often linked to systemic illness, nutritional stress, severe laminitis, trauma, or coronary band injury (Pollitt, 2008; Dyson, 2011). These cracks may appear as grooves or full-thickness defects and often migrate distally as the hoof grows (Leach, 2016).
Unlike vertical cracks, horizontal cracks are not typically load-bearing in nature, but they can predispose the wall to further breakdown, particularly if they weaken the structural integrity of the capsule (Parks, 2012). The presence of multiple horizontal defects may indicate repeated episodes of stress or illness, highlighting the importance of a thorough history when assessing affected horses (Dyson, 2011).

Complete and Incomplete Cracks
Incomplete cracks involve only a portion of the height of the hoof wall thickness and do not extend the full length of the hoof wall. These cracks are generally non-painful and may be detected incidentally during routine farriery (O’Grady, 2019). While often considered cosmetic, incomplete cracks can propagate if mechanical stresses persist (Leach, 2016).
Complete cracks extend through the full length of the hoof wall, potentially involving the sensitive structures found within the coronary band (Parks, 2012). These cracks compromise the hoof’s ability to bear weight and are more likely to be associated with pain, instability, and secondary infection (Dyson, 2011). Complete cracks require prompt and carefully planned intervention to prevent further deterioration.
Sensitive and Non-Sensitive Cracks
Non-sensitive cracks do not involve the sensitive laminae and are typically non-painful. The horse may remain sound, and digital pulses are usually normal (Stashak and Hill, 2014). However, non-sensitive cracks should not be dismissed, as they can deepen over time if underlying causes are not addressed (O’Grady, 2019).
Sensitive cracks involve penetration or compression of the sensitive laminae, resulting in pain, inflammation, and sometimes infection (Pollitt, 2008). Horses with sensitive cracks may show varying degrees of lameness, increased digital pulses, localised heat, or reluctance to load the affected limb (Dyson, 2011). Sensitive cracks often necessitate veterinary involvement, particularly if infection or instability of the distal phalanx is suspected.

Toe Cracks
Toe cracks are vertical cracks located at the dorsal aspect of the hoof wall. They commonly originate at the coronary band and extend distally, although some may begin at the distal border of the hoof wall and migrate proximally (Parks, 2012). Toe cracks are frequently associated with excessive toe length, delayed breakover, and increased tensile forces on the dorsal wall (Clayton and Hobbs, 2017).
Biomechanically, the toe region experiences significant stress during breakover. If the hoof is allowed to become long in the toe, leverage forces increase, predisposing the wall to failure (O’Grady and Poupard, 2013). Toe cracks may also be associated with previous laminitic episodes, as compromised lamellar attachments reduce the wall’s ability to withstand load (Pollitt, 2008).
Quarter Cracks
Quarter cracks occur in the medial or lateral quarter of the hoof and are among the most clinically significant forms of hoof wall cracking (Dyson, 2011). They are often associated with instability of the hoof capsule, uneven loading, or poor heel support (O’Grady, 2019). The quarters are designed to expand and contract during weight-bearing, and any restriction or asymmetry in this movement can concentrate stress (Clayton et al., 2011).
Quarter cracks frequently become sensitive due to the proximity of weight-bearing structures and the dynamic nature of the region (Parks, 2012). They may be unilateral or bilateral and are often linked to conformational issues such as base-narrow or base-wide limb alignment, as well as shoeing practices that restrict hoof expansion (Leach, 2016).

Causes of Hoof Wall Cracks
The causes of hoof wall cracks are multifactorial and can be broadly divided into mechanical, environmental, nutritional, and pathological factors (O’Grady and Poupard, 2013). Mechanical causes include poor hoof balance, long toes, under-run heels, mediolateral imbalance, and inappropriate shoeing (Parks, 2012). Environmental factors such as excessive moisture, prolonged dryness, or frequent changes between the two can weaken horn quality (Faramarzi et al., 2020).
Nutritional deficiencies, particularly of biotin, zinc, copper, and essential amino acids, can impair horn production and strength (Geor et al., 2013). Pathological causes include laminitis, white line disease, trauma to the coronary band, and chronic infection (Pollitt, 2008). In many cases, cracks develop as the result of several interacting factors rather than a single identifiable cause.
Clinical Signs and Symptoms
The clinical presentation of hoof wall cracks varies depending on their type and severity (Dyson, 2011). Superficial, non-sensitive cracks may present with minimal clinical signs beyond visible wall defects. In contrast, sensitive or unstable cracks may be associated with lameness, shortened stride length, uneven gait, and reluctance to turn or work on certain surfaces (Stashak and Hill, 2014).
Local signs may include increased digital pulses, heat in the hoof capsule, and tenderness on hoof tester examination (Parks, 2012). In chronic cases, secondary infection may result in discharge, malodour, or granulation tissue formation. Observing the horse both at rest and in motion is essential to fully appreciate the functional impact of the crack (Clayton and Hobbs, 2017).
Visual Assessment: Static Examination
Static assessment begins with careful observation of the horse standing square on a level surface (O’Grady, 2019). The farrier should assess limb conformation, hoof symmetry, wall alignment, and coronary band integrity. The location, length, width, and orientation of the crack should be noted, along with any associated flares, distortions, or dishing of the wall (Parks, 2012).
The coronary band should be examined for signs of injury, scarring, or uneven horn production, particularly in cases of vertical cracks originating proximally (Pollitt, 2008). Solar examination provides additional information regarding hoof balance, white line integrity, and potential areas of overload that may contribute to crack formation (Leach, 2016).
Visual Assessment: Dynamic Examination
Dynamic assessment involves observing the horse in motion, both in straight lines and on circles, on firm and compliant surfaces (Clayton and Hobbs, 2017). Particular attention should be paid to landing patterns, breakover timing, and mediolateral loading (Clayton et al., 2011). Horses with hoof wall cracks may exhibit toe-first or uneven landings, reflecting discomfort or mechanical imbalance (Dyson, 2011).
Slow-motion observation, where possible, can assist in identifying subtle gait abnormalities. The relationship between the crack location and phases of the stride cycle often provides valuable insight into the forces contributing to the defect (Clayton and Hobbs, 2017). Dynamic assessment is essential in guiding trimming and shoeing decisions aimed at redistributing load.
Veterinary Diagnostics
Veterinary involvement is particularly important in cases involving sensitive cracks, lameness, or suspected internal pathology (Dyson, 2011). Diagnostic analgesia may be used to localise pain, while radiography can assess the position of the distal phalanx, wall thickness, and the presence of gas lines or infection tracking along the laminae (Parks, 2012). Radiography also plays an important role in establishing a trimming and shoeing plan should there be any hoof imbalances present.
Advanced imaging, such as ultrasonography or computed tomography, may be employed in complex cases to evaluate soft tissue involvement or subtle bony changes (Dyson, 2011). Collaboration between farrier and veterinarian ensures that treatment strategies address both mechanical and pathological components of the condition.
Trimming Principles in Crack Management
Corrective trimming is central to the management of hoof wall cracks (O’Grady and Poupard, 2013). The primary objectives are to restore hoof balance, reduce abnormal stresses on the affected area, and promote the growth of strong, well-aligned horn from the coronary band (Parks, 2012). Excessive toe length should be addressed to reduce leverage forces, and mediolateral balance should be optimised to ensure even load distribution.
Flare associated with cracks should be carefully reduced without weakening the wall further (Leach, 2016). Over-aggressive removal of horn is contraindicated, particularly in cases of complete or sensitive cracks. Regular, conservative trimming at appropriate intervals is preferable to infrequent, extensive intervention (O’Grady, 2019).
Shoeing Options and Farriery Interventions
Shoeing strategies aim to stabilise the hoof capsule, offload the cracked region, and support physiological movement (Parks, 2012). Options may include the use of full-support shoes, bar shoes, or shoes with modified branches to redistribute load away from the affected area (O’Grady and Poupard, 2013). In some cases, shoeing without nails in the immediate vicinity of the crack is advisable to prevent further wall separation (Leach, 2016).
Adjunctive techniques such as lacing, patching, or the use of composite materials may be employed to stabilise the crack and prevent propagation (O’Grady, 2019). These methods should be used judiciously and in conjunction with appropriate trimming and shoeing, rather than as standalone solutions. The choice of intervention should be tailored to the individual horse, discipline, and severity of the crack.


Long-Term Management and Prognosis
The long-term prognosis for horses with hoof wall cracks depends on the type, severity, and underlying causes of the condition (Dyson, 2011). Superficial, non-sensitive cracks often have an excellent prognosis with appropriate farriery and management. More severe cracks, particularly chronic quarter cracks or those associated with laminitis, may require prolonged treatment and carry a more guarded prognosis (Pollitt, 2008).
Successful long-term management relies on consistent farriery, attention to nutrition and environment, and ongoing monitoring of hoof balance and horn quality (Geor et al., 2013). Education of the owner or trainer is also crucial, as management practices such as turnout conditions and shoeing intervals significantly influence outcomes.
Conclusion
Hoof wall cracks represent a multifaceted challenge within equine farriery, requiring a thorough understanding of hoof anatomy, biomechanics, and pathology (Parks, 2012). Accurate classification, careful assessment, and evidence-based intervention are essential to achieving successful outcomes. By addressing both the mechanical and biological factors contributing to crack formation, farriers play a central role in restoring hoof integrity and maintaining equine soundness. Through collaborative practice and a long-term perspective, even complex cases can be effectively managed, preserving the health and performance of the horse.
References
Bowker, R.M. (2003) ‘Contrasting structural morphologies of the equine digital cushion in young and mature horses’, Equine Veterinary Journal, 35(6), pp. 612–618.
Clayton, H.M. and Hobbs, S.J. (2017) The Dynamic Horse: A Biomechanical Guide to Equine Movement and Performance. 2nd edition. Mason, MI: Sport Horse Publications.
Clayton, H.M., Hobbs, S.J. and Richards, J. (2011) ‘The effect of hoof angle on equine locomotion’, Equine Veterinary Journal, 43(1), pp. 16–23.
Dyson, S.J. (2011) Diagnosis and Management of Lameness in the Horse. 2nd edition. St. Louis: Elsevier.
Faramarzi, B., Eslami, M. and Mohajer, A. (2020) ‘Environmental influences on equine hoof horn quality’, Journal of Equine Veterinary Science, 89, 103084.
Geor, R.J., Harris, P.A. and Coenen, M. (2013) Equine Applied and Clinical Nutrition. Edinburgh: Saunders Elsevier.
Leach, D. (2016) ‘Hoof wall defects and their management’, Equine Veterinary Education, 28(7), pp. 370–377.
Leach, D. and Zoerb, G. (2014) ‘Mechanical properties of the equine hoof wall’, Journal of Equine Veterinary Science, 34(1), pp. 34–41.
O’Grady, S.E. (2019) ‘Managing hoof wall defects in the performance horse’, Veterinary Clinics of North America: Equine Practice, 35(2), pp. 353–370.
O’Grady, S.E. and Poupard, D.A. (2013) ‘Physiology and management of the hoof wall’, Veterinary Clinics of North America: Equine Practice, 29(2), pp. 371–386.
Parks, A.H. (2012) ‘Form and function of the equine digit’, Veterinary Clinics of North America: Equine Practice, 28(2), pp. 273–292.
Pollitt, C.C. (2004) ‘Equine laminitis’, Clinical Techniques in Equine Practice, 3(1), pp. 34–44.
Pollitt, C.C. (2008) ‘The anatomy and physiology of the suspensory apparatus of the distal phalanx’, Equine Veterinary Education, 20(6), pp. 331–338.
Stashak, T.S. and Hill, C. (2014) Adams’ Lameness in Horses. 6th edition. Oxford: Wiley-Blackwell.

Comments