
Cushings Disease in the Horse: A Complete Overview
- Marc Jerram

- Mar 8
- 8 min read
Introduction
Cushings disease in the horse, correctly termed pituitary pars intermedia dysfunction, represents one of the most significant chronic endocrine disorders encountered by farriers, veterinarians, and owners alike (McGowan and McGowan, 2017). Its importance within farriery cannot be overstated, as it is strongly associated with laminitis, progressive deterioration in hoof horn quality, delayed healing, and complex long term management challenges (Belknap, 2018). As advances in nutrition, veterinary medicine, and general husbandry have extended the lifespan of the domestic horse, conditions associated with ageing have become increasingly prevalent. Cushings disease is therefore no longer an uncommon diagnosis but a routine consideration in the assessment of older horses and ponies (Ireland et al., 2012).
For the farrier, Cushings disease demands a depth of understanding that goes beyond surface clinical signs. The disorder influences the horse systemically, altering metabolic balance, immune competence, vascular regulation, and tissue integrity (McFarlane, 2011). These changes are often reflected first and most clearly within the hoof. A farrier may therefore be the first professional to suspect the presence of the disease, particularly when faced with unexplained laminitic episodes, persistent hoof capsule distortion, or repeated foot infections in an older horse (Pollitt, 2016).
Prefer an audio version? Click the link below:
Understanding Cushings Disease in the Horse
Cushings disease in horses arises from dysfunction within the pituitary gland, specifically the pars intermedia. In the healthy horse, the pars intermedia is tightly regulated by dopamine released from neurons in the hypothalamus. Dopamine acts as an inhibitory neurotransmitter, suppressing excessive hormone production and maintaining endocrine balance (McFarlane et al., 2005). In Cushings disease, these dopaminergic neurons undergo progressive degeneration. As inhibitory control is lost, the pars intermedia becomes hyperplastic and hyperactive (Schott, 2019).
This overactivity results in excessive production of proopiomelanocortin derived peptides, including adrenocorticotropic hormone and related hormones such as alpha melanocyte stimulating hormone and beta endorphins (Donaldson et al., 2002). These hormones have wide ranging effects throughout the body. While adrenocorticotropic hormone is classically associated with cortisol production in other species, in the horse the endocrine interactions are more complex and do not always result in sustained hypercortisolaemia (Durham et al., 2014). Nevertheless, the resulting hormonal imbalance profoundly disrupts metabolic regulation, immune function, thermoregulation, and vascular tone.
For the farrier, the relevance of this pathology lies in its chronic and progressive nature. Cushings disease is not an acute illness but a slowly advancing neurodegenerative condition (McFarlane, 2011). Over time, hormonal dysregulation affects the laminar tissues of the foot, compromises hoof horn quality, and alters the horse’s capacity to respond to both mechanical and metabolic stress (Belknap, 2018). Appreciating this progressive trajectory is essential when planning long term hoof care strategies and setting realistic expectations for owners.
Thorough Assessment of the Horse
Thorough assessment of a horse suspected of Cushings disease requires a holistic and methodical approach. The farrier’s assessment often begins with observation, sometimes long before a formal diagnosis is made. Many horses with Cushings disease present initially with subtle changes that may be dismissed as normal ageing unless carefully evaluated (Ireland et al., 2012).
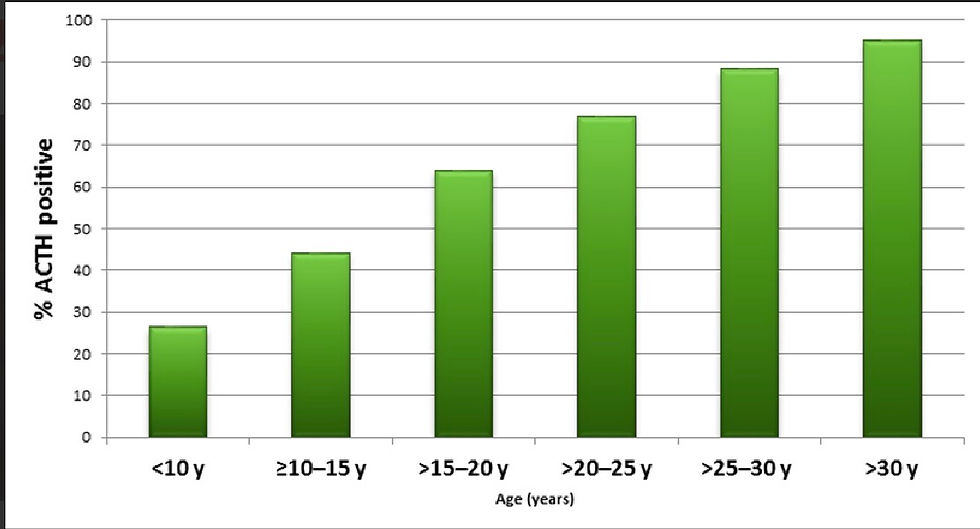
A comprehensive history is the foundation of assessment. Age is a critical factor, as the majority of affected horses are over fifteen years old, with prevalence increasing markedly in older populations (McGowan and McGowan, 2017). The farrier should enquire about previous episodes of laminitis, even if mild or self resolving, as recurrent low grade laminitis is a common early manifestation (Karikoski et al., 2011). Changes in coat shedding patterns, such as delayed shedding in spring or retention of long hair patches, should be noted, alongside alterations in body condition, exercise tolerance, and demeanour.

Static assessment provides valuable information about systemic health. Horses with Cushings disease frequently display muscle wastage along the topline and hindquarters, producing a hollowed appearance despite adequate nutrition (Schott, 2019). At the same time, fat deposition may occur in specific regions such as above the eyes, along the crest of the neck, or around the tail head. This combination of muscle loss and regional adiposity is characteristic of endocrine dysfunction. Postural changes, including a tendency to stand with the forelimbs camped out, may indicate chronic laminitic discomfort (Pollitt, 2016).

Dynamic assessment is essential for identifying subtle lameness or altered movement patterns. Horses with early laminitis associated with Cushings disease may not show overt lameness but often demonstrate shortened stride length, reluctance to turn, or stiffness on hard ground (Belknap, 2018). Observing the horse on different surfaces and at varying speeds allows the farrier to detect minor gait abnormalities that may otherwise be overlooked.
Hoof assessment is central to the farrier’s role. Cushings disease often results in slow and poor quality horn growth, increased brittleness of the hoof wall, and susceptibility to cracking and white line separation (O’Grady and Parks, 2008). Growth rings may be uneven or divergent, reflecting episodes of metabolic stress or subclinical laminitis. Sole depth is frequently reduced, increasing vulnerability to bruising, while digital pulse strength and hoof temperature may rise before overt laminitis becomes apparent (Pollitt, 2016).
Causes of Cushings Disease
The primary cause of Cushings disease in the horse is age related degeneration of dopaminergic neurons within the hypothalamus (McFarlane et al., 2005). This degeneration is believed to be driven largely by cumulative oxidative stress. As antioxidant defence mechanisms decline with age, neurons become increasingly vulnerable to oxidative damage, resulting in progressive loss of dopamine production (McFarlane, 2011).
While ageing is the dominant risk factor, other influences may contribute to disease expression. Genetic susceptibility has been proposed, as certain breeds and bloodlines appear overrepresented, although definitive genetic markers have yet to be identified (Ireland et al., 2012). Environmental stressors may further exacerbate disease progression by increasing oxidative burden and endocrine demand.
Dietary management also plays an indirect but clinically important role. Horses consuming diets high in non structural carbohydrates may develop insulin dysregulation, which frequently coexists with Cushings disease (Karikoski et al., 2011). While insulin dysregulation does not cause Cushings disease, it significantly amplifies laminitis risk and worsens clinical outcomes. Cushings disease should therefore be considered within the wider framework of equine metabolic health rather than as an isolated condition.
Clinical Signs of Cushings Disease
The clinical signs of Cushings disease are diverse and typically develop gradually, making early recognition challenging. One of the most widely recognised signs is abnormal hair coat. Affected horses may exhibit delayed shedding, patchy retention of winter coat, or development of a long, thick, and sometimes curly coat that persists year round (Schott, 2019). In early disease, these changes may be subtle and inconsistent.

Lethargy and reduced exercise tolerance are common but nonspecific signs. Horses may appear dull, unwilling to work, or slow to recover after exercise. Progressive muscle wastage, particularly along the topline, reflects altered protein metabolism and reduced anabolic hormone influence (McFarlane, 2011). Despite muscle loss, some horses maintain or gain weight due to altered fat distribution.
Laminitis is the most clinically significant manifestation of Cushings disease. Presentation ranges from acute, severe laminitic episodes to chronic, low grade laminitis that progressively undermines hoof integrity (Belknap, 2018). Recurrent hoof abscessation is also common and is believed to result from compromised laminar attachment, impaired immune function, and poor horn quality (Pollitt, 2016).
Additional signs include increased thirst and urination, excessive sweating, delayed wound healing, and recurrent infections. Collectively, these signs reflect widespread endocrine and immune dysfunction (Durham et al., 2014).

Use of Veterinary Diagnostics
Veterinary diagnosis of Cushings disease relies on integration of clinical findings with laboratory testing. Measurement of circulating adrenocorticotropic hormone concentration is the most commonly employed diagnostic test (Schott, 2019). Interpretation is complicated by marked seasonal variation, with higher concentrations observed in late summer and autumn, necessitating the use of seasonally adjusted reference ranges (Durham et al., 2014).
Where basal hormone concentrations are equivocal, dynamic testing such as the thyrotropin releasing hormone stimulation test may be performed. This test is regarded as highly sensitive, particularly for early disease, as affected horses demonstrate an exaggerated hormonal response (McFarlane, 2011).
Concurrent assessment of insulin and glucose dynamics is often indicated, particularly in horses with laminitis. Identification of insulin dysregulation is critical for targeted dietary and management interventions (Karikoski et al., 2011).
Radiography plays an essential supportive role in horses with hoof involvement. Imaging allows assessment of distal phalanx position, sole depth, and chronic laminitic changes, providing critical information for farriery planning and ongoing monitoring (O’Grady and Parks, 2008).
Learn more about radiography at the link below:
Veterinary Treatment
The primary veterinary treatment for Cushings disease is pharmacological management aimed at restoring dopaminergic inhibition of the pars intermedia. Pergolide mesylate is the treatment of choice and has been shown to reduce hormone production and improve clinical signs in the majority of affected horses (Donaldson et al., 2002).
Treatment is lifelong, as Cushings disease is progressive and incurable. Dosage must be individualised and adjusted according to clinical response and follow up hormone testing (Schott, 2019). Many horses demonstrate marked improvement in coat shedding, energy levels, and laminitis control once stabilised on treatment.
Transient side effects such as inappetence or lethargy may occur during initiation of therapy but can often be mitigated by gradual dose escalation (Durham et al., 2014). Comprehensive veterinary management also includes dental care, parasite control, vaccination, and nutritional optimisation, reinforcing the need for multidisciplinary collaboration.
Laminitis Risk and Farriery Management
Laminitis represents the most serious and farrier relevant complication of Cushings disease. Risk arises from the combined effects of endocrine imbalance, insulin dysregulation, and altered digital vascular control (Belknap, 2018). Even well managed horses remain at increased risk compared to unaffected individuals.
Farriery management focuses on reducing mechanical stress on compromised laminar tissues. Regular trimming is essential to maintain optimal hoof balance and reduce leverage forces, particularly at the toe (O’Grady and Parks, 2008). Radiographic guidance is invaluable in aligning the hoof capsule with the distal phalanx in horses with chronic laminitis.
Sole protection is frequently required due to reduced sole depth and increased sensitivity. Early detection of subtle laminitic indicators and prompt veterinary communication are critical in preventing progression to catastrophic structural failure (Pollitt, 2016).
Alternative Herbal Supplementation
Interest in alternative and herbal supplementation for Cushings disease has increased, often driven by owner concerns regarding lifelong pharmaceutical therapy. Many products claim to support pituitary function or antioxidant status. However, scientific evidence supporting their efficacy remains limited and inconsistent (Schott, 2019).
Herbal supplementation should not replace evidence based veterinary treatment. When used, it should be under veterinary supervision due to potential interactions with prescribed medication. The farrier’s observations of hoof quality and laminitis incidence remain essential in evaluating management effectiveness.
Long Term Prognosis
Long term prognosis varies widely depending on age at diagnosis, disease severity, response to treatment, and laminitic history. Early diagnosis and timely initiation of therapy significantly improve outcomes (McGowan and McGowan, 2017).
Many horses maintain a good quality of life for years when appropriately managed. However, horses with chronic laminitis may require intensive lifelong care. As Cushings disease is progressive, ongoing reassessment and adaptation of both veterinary and farriery strategies are essential.
Conclusion
Cushings disease is a complex, progressive endocrine disorder with profound implications for hoof health and long term welfare. Through informed assessment, vigilant monitoring, and close collaboration with veterinary colleagues, farriers play a central role in maintaining comfort and quality of life in affected horses. With evidence based, compassionate management, Cushings disease need not preclude long term soundness or dignity in old age.
References
Belknap, J.K. (2018) Equine Laminitis. 2nd edn. Hoboken: Wiley Blackwell.
Donaldson, M.T., LaMonte, B.H., Morresey, P., Smith, G. and Beech, J. (2002) Treatment with pergolide or cyproheptadine of pituitary pars intermedia dysfunction in horses. Journal of the American Veterinary Medical Association, 221(12), pp. 1733–1736.
Durham, A.E., McGowan, C.M., Fey, K. and Tamzali, Y. (2014) Pituitary pars intermedia dysfunction: diagnosis and management. Equine Veterinary Education, 26(4), pp. 216–223.
Ireland, J.L., Clegg, P.D., McGowan, C.M., McKane, S.A., Chandler, K.J. and Pinchbeck, G.L. (2012) A cross sectional study of geriatric horses in the United Kingdom. Equine Veterinary Journal, 44(1), pp. 101–106.
Karikoski, N.P., Horn, I., McGowan, T.W., McGowan, C.M. and Pollitt, C.C. (2011) Lamellar pathology in horses with pituitary pars intermedia dysfunction. Equine Veterinary Journal, 43(1), pp. 80–85.
McFarlane, D. (2011) Equine pituitary pars intermedia dysfunction. Veterinary Clinics of North America: Equine Practice, 27(1), pp. 93–113.
McFarlane, D., Dybdal, N. and Donaldson, M. (2005) Nitration and degeneration of dopaminergic neurons in pituitary pars intermedia dysfunction. Journal of Neuroendocrinology, 17(2), pp. 73–80.
McGowan, C.M. and McGowan, T.W. (2017) Endocrine disorders of the geriatric horse. Veterinary Clinics of North America: Equine Practice, 33(1), pp. 127–143.
O’Grady, S.E. and Parks, A.H. (2008) Farriery for chronic laminitis. Veterinary Clinics of North America: Equine Practice, 24(2), pp. 461–477.
Pollitt, C.C. (2016) The Anatomy and Physiology of the Suspensory Apparatus of the Distal Phalanx. Queensland: RIRDC.
Schott, H.C. (2019) Pituitary pars intermedia dysfunction in horses. Merck Veterinary Manual.


Comments