
Navicular Syndrome
- Marc Jerram

- May 17
- 11 min read
Introduction
Navicular syndrome remains one of the most important causes of chronic forelimb lameness in horses and continues to represent a major challenge within equine veterinary medicine and farriery practice. Historically referred to as navicular disease, the condition was once believed to involve degeneration of the navicular bone alone. Modern research has demonstrated that the syndrome is considerably more complex and includes pathological changes involving the navicular bone, deep digital flexor tendon, navicular bursa, distal sesamoidean impar ligament and associated soft tissues within the caudal aspect of the equine foot (Dyson and Murray, 2007).
The condition is particularly common in performance horses involved in disciplines requiring repetitive concussion and increased loading of the forelimbs such as showjumping, dressage and eventing (Turner, 2012). Horses with poor hoof balance, long toes and underrun heels appear predisposed due to abnormal biomechanical forces acting upon the navicular apparatus (O Grady and Poupard, 2003). Navicular syndrome significantly affects athletic performance, welfare and long term soundness, making its understanding essential for both veterinary surgeons and farriers.
Advances in diagnostic imaging, particularly magnetic resonance imaging, have greatly improved understanding of the syndrome. These technologies have revealed that many horses suffering from navicular related lameness possess significant soft tissue injury despite relatively minor radiographic changes of the navicular bone itself (Dyson et al., 2011). Consequently modern therapeutic approaches focus upon management of the entire navicular apparatus rather than solely the distal sesamoid bone.
Farriery remains central to the prevention and management of navicular syndrome. Appropriate trimming and shoeing can improve hoof biomechanics, reduce tension within the deep digital flexor tendon and provide enhanced support to the caudal foot (Moyer and Schumacher, 2019). Conversely poor farriery can exacerbate pathology through delayed breakover, heel collapse and excessive stress upon sensitive structures.
Prefer an audio version? Listen at the link below:
Anatomy of the Navicular Bone and Navicular Apparatus
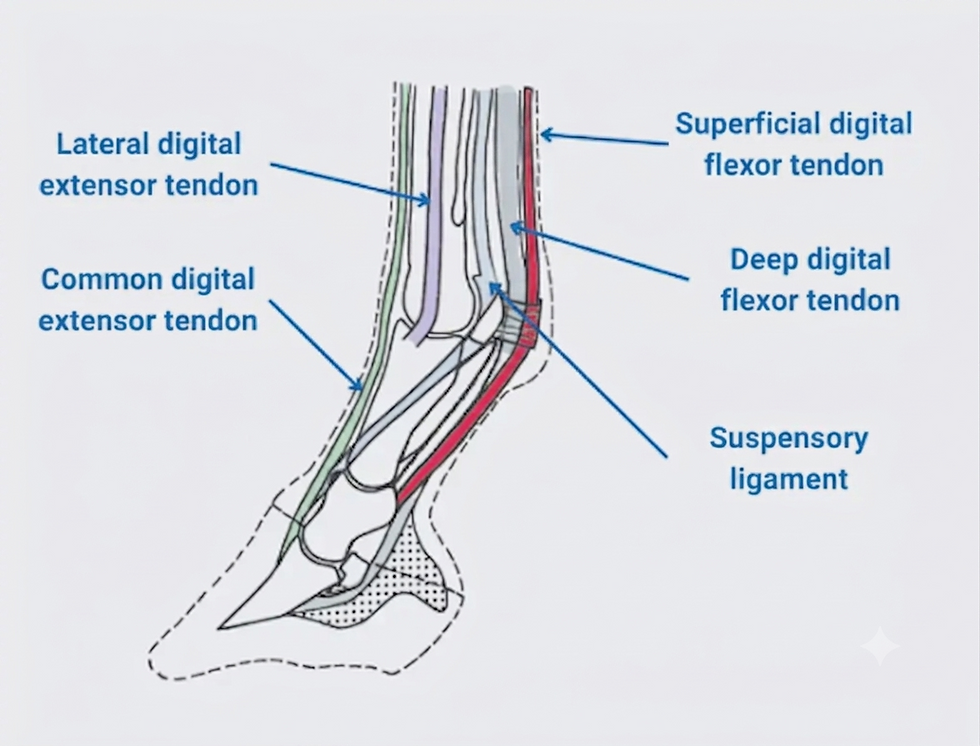
The navicular bone, also known as the distal sesamoid bone, is a small elongated structure located on the palmar aspect of the distal interphalangeal joint between the middle phalanx and distal phalanx. The bone acts as a fulcrum over which the deep digital flexor tendon passes before inserting onto the solar surface of the distal phalanx (Ross and Dyson, 2011).
The navicular bone possesses several distinct anatomical surfaces. The flexor surface lies adjacent to the deep digital flexor tendon and is covered by fibrocartilage which reduces friction during locomotion. The articular surface faces dorsally and articulates with the distal interphalangeal joint. Numerous vascular channels penetrate the bone and are visible radiographically. Historically alterations in these channels were considered hallmarks of navicular disease although their diagnostic significance is now interpreted with caution (Powell, 2017).
The navicular bone is stabilised by several ligamentous structures. The collateral sesamoidean ligaments suspend the bone proximally while the distal impar ligament anchors it distally to the distal phalanx. The navicular bursa lies between the deep digital flexor tendon and the flexor surface of the navicular bone and functions to minimise friction during movement (Dyson and Murray, 2007).
The hoof capsule plays an essential role in supporting the navicular apparatus. During weight bearing the frog, digital cushion and heels absorb concussion and dissipate forces generated during locomotion. Horses with poor hoof conformation such as underrun heels and long toes experience increased tension within the deep digital flexor tendon and elevated pressure against the navicular bone (O Grady and Poupard, 2003).
Blood supply to the navicular bone is relatively limited compared with many skeletal structures. Compromised vascular perfusion may contribute to degeneration and impaired tissue repair within the navicular apparatus (Waguespack and Hanson, 2010).
Signs of Navicular Syndrome
Clinical signs associated with navicular syndrome are often subtle during the early stages of disease progression. Affected horses commonly present with intermittent forelimb lameness that gradually becomes more consistent over time (Ross and Dyson, 2011).
Many horses exhibit bilateral forelimb involvement resulting in a short choppy gait rather than an obvious unilateral lameness. Riders frequently report stumbling, reluctance to move forwards and decreased performance, particularly on hard ground or during turning movements (Turner, 2012).
One characteristic feature involves toe first landing during locomotion. Healthy horses normally land heel first, allowing the frog and digital cushion to absorb concussion effectively. Horses suffering from navicular pain attempt to reduce loading of the caudal foot by avoiding heel contact, thereby altering normal hoof mechanics (Moyer and Schumacher, 2019).
Affected horses may point one forelimb forwards while standing in order to relieve pressure upon the heels. Hoof tester examination across the frog and heel region often elicits pain responses although findings may vary considerably between individuals (Dyson et al., 2011).
Chronic cases frequently demonstrate contracted heels, narrow frogs and long toe low heel conformation. Secondary muscular asymmetry may develop through prolonged compensation and altered gait patterns (Powell, 2017).
Causes of Navicular Syndrome
Navicular syndrome possesses a multifactorial aetiology involving conformation, biomechanics, workload, genetics and environmental influences. No single factor is responsible for all cases and the condition generally develops through cumulative stress over time (Ross and Dyson, 2011).
Poor hoof balance is considered one of the most important contributing factors. Horses with long toes and underrun heels experience delayed breakover and increased tension within the deep digital flexor tendon. This results in elevated compressive forces acting upon the navicular apparatus (O Grady and Poupard, 2003).
Conformation also influences susceptibility. Horses possessing upright pasterns and feet absorb less concussion through the limb while horses with small feet relative to body mass experience greater focal loading within the hoof capsule (Turner, 2012).
Repetitive concussion associated with athletic activity on hard surfaces contributes significantly to degeneration. Performance horses involved in jumping disciplines experience substantial loading forces during landing which may predispose them to navicular related injury (Murray et al., 2006).
Improper farriery may exacerbate pathological change. Excessively long shoeing intervals, shoes positioned too far forwards and inadequate heel support can all increase biomechanical stress within the navicular region (Moyer and Schumacher, 2019).
Genetic predisposition has also been proposed. Certain Warmblood and Quarter Horse bloodlines appear overrepresented among affected populations although precise hereditary mechanisms remain poorly understood (Dyson and Murray, 2007).
Pathogenesis of Navicular Syndrome
The pathogenesis of navicular syndrome involves chronic biomechanical stress resulting in progressive degeneration of structures within the navicular apparatus. Modern evidence suggests that pathology affecting the deep digital flexor tendon and associated soft tissues is often equally or more important than osseous change within the navicular bone itself (Dyson et al., 2011).
Long toe low heel conformation increases tension within the deep digital flexor tendon during breakover. As the tendon passes over the flexor surface of the navicular bone, excessive compressive forces develop between the two structures (O Grady and Poupard, 2003).
Repeated loading damages fibrocartilage upon the flexor surface and promotes inflammation within the navicular bursa. Microtearing and degeneration of tendon fibres commonly develop near the level of the navicular bone (Ross and Dyson, 2011).
Chronic inflammation and vascular compromise may contribute to bone remodelling. Radiographic changes including medullary sclerosis, enlarged vascular channels and cortical erosions reflect attempts at adaptation and repair (Powell, 2017).
Pain originating from the navicular region alters gait mechanics. Horses adopt toe first landing patterns which reduce heel loading but simultaneously increase stress upon the dorsal hoof wall and deep digital flexor tendon. Secondary hoof capsule distortion and heel contraction consequently develop, perpetuating abnormal biomechanics (Moyer and Schumacher, 2019).
Dietary Considerations
Nutrition plays a supportive role in the management of navicular syndrome. Although dietary modification cannot cure the disease, appropriate nutrition may improve hoof quality, reduce inflammation and assist weight management (Geor et al., 2013).
Maintaining ideal body condition is essential because excessive body weight increases loading upon the distal limbs and navicular apparatus. Controlled calorie intake and regular exercise therefore form important components of long term management (Ralston, 2011).
Hoof horn quality depends upon adequate intake of biotin, methionine, zinc and copper. Deficiencies in these nutrients may compromise hoof integrity and reduce shock absorption capacity (Pagan, 2018).
Omega three fatty acids derived from linseed may provide anti inflammatory benefits through modulation of inflammatory mediators. Reduction of excessive dietary starch and sugar may also help minimise systemic inflammation and maintain metabolic stability (Geor et al., 2013).
Adequate hydration supports hoof elasticity and horn quality. Horses consuming predominantly dry forage may require careful monitoring to ensure sufficient water intake particularly during warm weather or periods of increased exercise (Pagan, 2018).
Veterinary Diagnostics
Diagnosis of navicular syndrome requires comprehensive clinical examination combined with advanced diagnostic imaging techniques. Because numerous conditions affecting the foot produce similar clinical signs, accurate localisation of pain is essential (Ross and Dyson, 2011).
Clinical examination includes gait analysis on hard and soft surfaces, flexion tests and hoof tester evaluation. Horses suffering from navicular syndrome frequently demonstrate increased lameness during circling movements on firm footing (Dyson et al., 2011).
Diagnostic analgesia plays an important role. Palmar digital nerve blocks commonly improve lameness associated with navicular related pain although they desensitise multiple structures within the foot and therefore cannot isolate specific pathology conclusively (Turner, 2012).
Radiography remains widely used for evaluation of the navicular bone. Common findings include enlarged vascular channels, flexor cortical erosions and medullary sclerosis. However radiographic abnormalities do not always correlate with clinical severity (Powell, 2017).

Magnetic resonance imaging has transformed understanding of navicular syndrome by allowing visualisation of both osseous and soft tissue structures. Lesions affecting the deep digital flexor tendon, navicular bursa and collateral ligaments can be identified accurately using this modality (Dyson et al., 2011).
Computed tomography and nuclear scintigraphy may also assist diagnosis in selected cases although these techniques are less commonly utilised in general practice (Ross and Dyson, 2011).
Veterinary Treatment
Veterinary treatment aims to reduce pain, minimise inflammation and slow progression of degeneration within the navicular apparatus. Most treatment plans involve a combination of medication, corrective farriery and exercise modification (Turner, 2012).
Non steroidal anti inflammatory drugs such as phenylbutazone are commonly administered to reduce pain and inflammation. Long term use requires careful monitoring due to potential adverse gastrointestinal and renal effects (Ross and Dyson, 2011).
Intra synovial medication of the distal interphalangeal joint or navicular bursa may provide significant relief. Corticosteroids reduce inflammation while hyaluronic acid improves synovial lubrication (Dyson and Murray, 2007).
Bisphosphonate medications including tiludronate and clodronate have become increasingly popular for management of navicular related pain. These drugs influence bone metabolism and may reduce discomfort associated with osseous remodelling (Denoix et al., 2012).
Regenerative therapies such as platelet rich plasma and stem cell treatment are currently being investigated for management of deep digital flexor tendon injury within the foot (Smith, 2016).
Palmar digital neurectomy may be considered in severe refractory cases. This surgical procedure eliminates sensation from the heel region through transection of the palmar digital nerves. Although some horses return to athletic function following surgery, complications including neuroma formation and recurrent lameness remain concerns (Turner, 2012).
Static Assessment of the Horse with Navicular Syndrome
Static assessment is an essential component of farriery evaluation. Observation of posture, conformation and hoof balance provides valuable insight into abnormal biomechanical forces affecting the navicular apparatus (Moyer and Schumacher, 2019).
Affected horses commonly point one forelimb forwards while standing. Frequent shifting of weight between limbs may also occur due to discomfort within the heels (O Grady and Poupard, 2003).
Hoof capsule symmetry should be evaluated carefully. Horses with navicular syndrome frequently exhibit contracted heels, narrow frogs and long toe low heel conformation. Mediolateral imbalance may contribute to uneven loading within the foot (Powell, 2017).
Assessment of frog condition and digital cushion development is important because these structures play major roles in shock absorption and caudal foot support. Atrophy of the frog and digital cushion commonly accompanies chronic heel pain (Moyer and Schumacher, 2019).
Learn more about the frog here:
Dynamic Assessment of the Horse with Navicular Syndrome
Dynamic assessment evaluates gait abnormalities associated with navicular syndrome. Horses should be observed at walk and trot on multiple surfaces and during circling movements (Ross and Dyson, 2011).
Toe first landing represents one of the most important findings because it reflects avoidance of heel loading. Delayed breakover and shortened cranial phase limb movement are also common observations (Turner, 2012).
Video analysis and slow motion recording have become increasingly valuable tools within modern farriery practice because they allow detailed assessment of landing patterns and limb flight asymmetry (Moyer and Schumacher, 2019).
Dynamic assessment under saddle may reveal additional signs including stumbling,
reluctance to move forwards and resistance during collection or turning movements (Dyson et al., 2011).
Farriery Trimming and Shoeing Methods
Farriery management is one of the most important aspects of navicular syndrome treatment. The primary objectives include improving hoof balance, enhancing breakover and supporting the caudal foot while reducing stress upon the navicular apparatus (O Grady and Poupard, 2003).
Trimming should aim to shorten the toe appropriately while preserving heel mass and maintaining adequate frog support. Excessive heel removal should be avoided because this increases tension within the deep digital flexor tendon (Moyer and Schumacher, 2019).
Raised heel shoeing has historically been used to reduce deep digital flexor tendon tension. Heel elevation may be achieved through wedge shoes or pads. However excessive elevation may weaken heel structures and should therefore be used cautiously (Turner, 2012).
Egg bar shoes provide increased support behind the heels and redistribute loading across the caudal foot. These shoes are commonly used in horses suffering from navicular syndrome because they improve stability and reduce focal pressure upon painful structures (O Grady and Poupard, 2003).

Memphis bar shoes incorporate frog support through a central bar positioned across the frog region. Increased frog loading may improve shock absorption and enhance weight distribution within the foot (Moyer and Schumacher, 2019).
Pads and impression materials may provide additional cushioning and support. Full pads can reduce concussion while impression materials distribute pressure more evenly across the solar surface (Turner, 2012).

Barefoot rehabilitation has gained increased interest in recent years. Carefully managed barefoot trimming may improve hoof function, heel expansion and frog development in selected horses. Hoof boots containing supportive pads are often used during transition periods to improve comfort and encourage heel first landing (Bowker, 2011).
No single shoeing method is appropriate for every horse because pathology and conformation vary considerably between individuals. Successful farriery requires regular reassessment and close collaboration between farrier and veterinarian (Moyer and Schumacher, 2019).
Learn more about hoof boots at the podcast link below:
Prognosis
The prognosis for horses suffering from navicular syndrome varies considerably depending upon severity, structures involved and response to treatment. Horses diagnosed during early stages generally possess more favourable long term outcomes (Ross and Dyson, 2011).
Mild cases may remain comfortable for many years with corrective farriery, controlled exercise and veterinary management. Horses with extensive deep digital flexor tendon injury or severe osseous degeneration possess a more guarded prognosis (Dyson et al., 2011).
Long term success depends heavily upon consistent hoof care, appropriate workload management and early intervention when clinical signs worsen. Although navicular syndrome is generally considered a chronic progressive condition, many horses can continue useful athletic careers with effective multidisciplinary management (Turner, 2012).
Conclusion
Navicular syndrome remains one of the most complex causes of chronic forelimb lameness in the horse. Modern understanding recognises that the condition involves a spectrum of pathological changes affecting the entire navicular apparatus rather than the navicular bone alone.
Poor hoof balance, conformational defects, repetitive concussion and abnormal biomechanics all contribute significantly to disease development and progression. Advances in diagnostic imaging have greatly improved identification of both osseous and soft tissue lesions within the foot.
Farriery plays a central role in management through restoration of hoof balance, improvement of breakover and support of the caudal foot. Therapeutic shoeing options including egg bar shoes, Memphis bar shoes, pads and supportive barefoot rehabilitation strategies may significantly improve comfort and function in affected horses.
Successful long term management requires collaboration between veterinarian, farrier and owner. Although navicular syndrome often carries a guarded prognosis, many horses can maintain acceptable comfort and athletic usefulness through appropriate multidisciplinary care.
References
Bowker, R.M. (2011) Contrasting structural morphologies of the peripheral foot in barefoot and traditionally shod horses. Equine Veterinary Education. 23(3), pp. 143 to 151.
Denoix, J.M., Thibaud, D. and Riccio, B. (2012) Tiludronate as a new therapeutic agent in the treatment of navicular disease. Equine Veterinary Journal. 44(2), pp. 210 to 216.
Dyson, S. and Murray, R. (2007) Navicular disease and associated disorders. Equine Veterinary Education. 19(1), pp. 27 to 35.
Dyson, S.J., Murray, R.C. and Branch, M.V. (2011) Magnetic resonance imaging of the equine foot. Equine Veterinary Education. 23(1), pp. 28 to 39.
Geor, R.J., Harris, P.A. and Coenen, M. (2013) Equine Applied and Clinical Nutrition. Edinburgh. Saunders Elsevier.
Moyer, W. and Schumacher, J. (2019) Equine Podiatry. St Louis. Elsevier.
Murray, R.C., Dyson, S.J., Schramme, M.C. and Branch, M.V. (2006) Magnetic resonance imaging findings in the deep digital flexor tendon in horses with navicular syndrome. Equine Veterinary Journal. 38(2), pp. 175 to 179.
O Grady, S.E. and Poupard, D.A. (2003) Proper physiologic horseshoeing for navicular syndrome. Veterinary Clinics of North America Equine Practice. 19(2), pp. 417 to 441.
Pagan, J.D. (2018) Advances in Equine Nutrition Volume V. Kentucky. Kentucky Equine Research.
Powell, D.M. (2017) Disorders of the navicular apparatus. Veterinary Clinics of North America Equine Practice. 33(1), pp. 87 to 104.
Ralston, S.L. (2011) Clinical nutrition of the performance horse. Veterinary Clinics of North America Equine Practice. 27(1), pp. 137 to 147.
Ross, M.W. and Dyson, S.J. (2011) Diagnosis and Management of Lameness in the Horse. 2nd edn. St Louis. Elsevier.
Smith, R.K.W. (2016) Regenerative medicine for tendon and ligament injuries of horses. Veterinary Clinics of North America Equine Practice. 32(1), pp. 95 to 123.
Turner, T.A. (2012) Navicular disease management in the performance horse. Equine Veterinary Education. 24(6), pp. 293 to 300.
Waguespack, R.W. and Hanson, R.R. (2010) Navicular syndrome in equine athletes. Compendium Equine. 5(4), pp. 1 to 11.

I find that the text demonstrates analytical restraint. The reasoning is clear and well-founded. The website adds depth and nuance to the issues raised here. Trend analysis is enriched by longitudinal platform usage data.